I was given the opportunity to enroll in this plan of group health benefits offered by my employer and insured by CIGNA. Children coverage Reason for Refusal Please check all appropriate boxes Other group coverage sponsored by my employer Other group coverage sponsored by my.
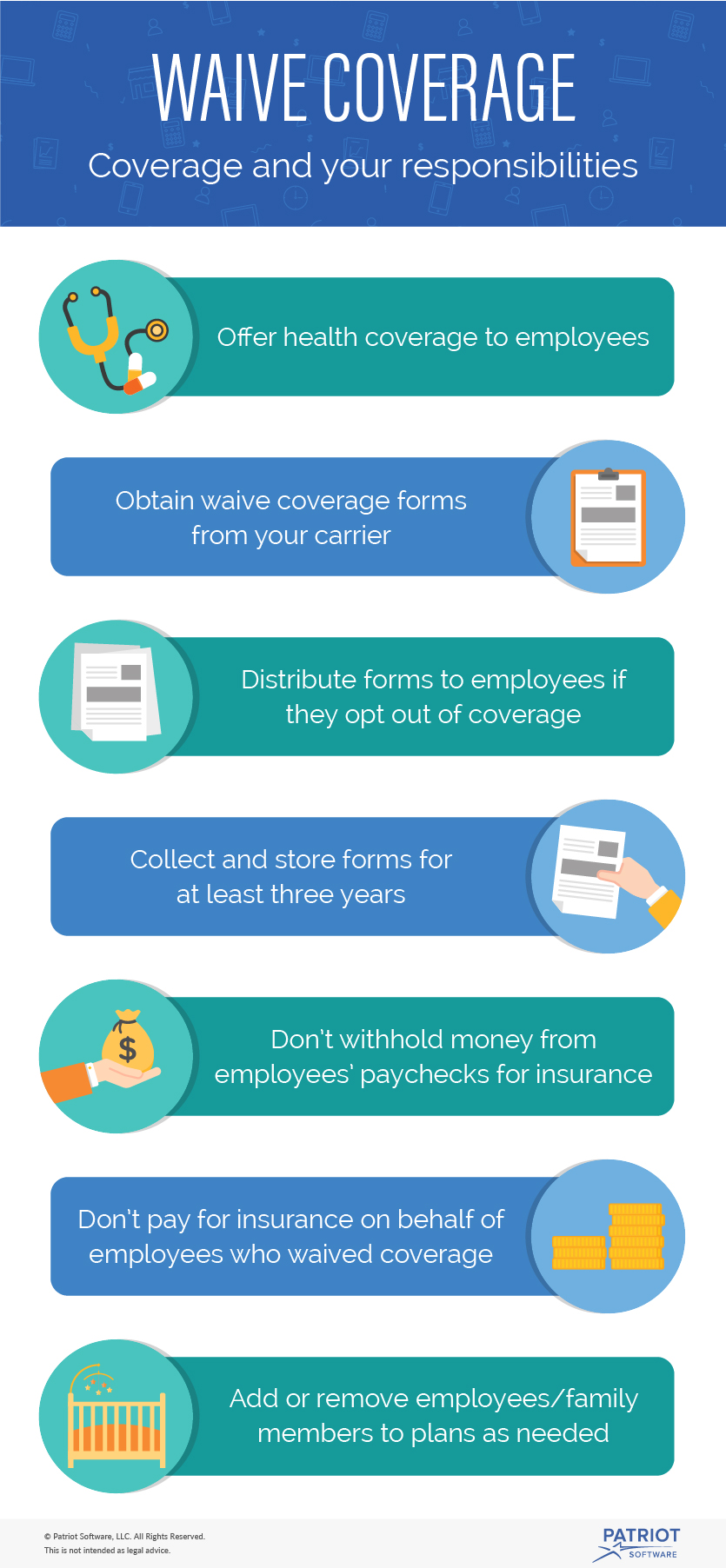 How To Handle Employees Who Want To Waive Health Insurance Coverage
How To Handle Employees Who Want To Waive Health Insurance Coverage
20201 1-800-368-1019 or 1-800-537-7697 TDD Complaint forms are available at wwwhhsgovocrofficefileindexhtml.

Small employer health benefits waiver of coverage. SMALL EMPLOYER HEALTH BENEFITS WAIVER OF COVERAGE CUSTOMER NAME I understand that if I wish to enroll for any of the coverage refused I will be required to submit an Enrollment Form. Horizon BCBSNJ Civil Rights Coordinator PO Box 820 Newark NJ 07101 You can also file a civil rights complaint with the US. If you fail to provide this information on this Waiver of Coverage form and you later become ineligible for such other coverage and then wish to enroll in any of the refused coverages you will be considered a Late Enrollee and may be subject to the pre-existing conditions exclusion.
If you fail to provide this information on this Waiver of Coverage form and you later become ineligible for such other coverage and then wish to enroll in any of the refused coverages. _____ Policyholder Name _____ Employee Name _____ Last First MI. Small Employer Health Benefits Waiver of Coverage You may complete the required fields below online and then save or print a copy for submission.
To save a completed copy to your computer choose File Save As to rename the file and save the form with your information to your computer. SOCIAL SECURITY DATE OF BIRTH DATE OF HIRE Month Day Year Month Day Year. SMALL EMPLOYER HEALTH BENEFITS WAIVER OF COVERAGE Group.
Signature of Employee EMPLOYEE NAME Last First MI. Box 7085 Bridgeport CT 06601-7085 800-385-9088. SMALL EMPLOYER HEALTH BENEFITS WAIVER OF COVERAGE GROUP NAME I understand that if I later wish to enroll for any of the coverages refused I will be required to submit an Enrollment Form and coverage may be subject to a pre-existing conditions exclusions.
Reason for Refusal Please check all appropriate boxes Other group coverage sponsored by my employer Other group coverage sponsored by my spouses. _____ Signature of Employee Date _____ Signature of Benefits Administrator Date Last First Middle Initial New Jersey Small Employer Health Benefits Waiver of Coverage Mailing Address. Signature of Benefits Administrator Date Last First Middle Initial New Jersey Small Employer Health Benefits Waiver of Coverage Mailing Address.
Signature of Employee BenefitsWaiverIBC EMPLOYEE NAME Last First MI. Small Employer Health Benefits Waiver of Coverage. Employee Spouse and Children coverage Spouse coverage Children coverage Reason for Refusal Please check all appropriate boxes.
Pre-Existing Conditions Statement and coverage may be subject to a pre-existing conditions exclusion. ___Single ___Married ___Widowed ___Divorced. I refuse the following.
___Single ___Married ___Widowed ___Divorced. I was given the opportunity to enroll in this plan of group health benefits offered by my employer and insured by AmeriHealth New Jersey. SMALL EMPLOYER HEALTH BENEFITS WAIVER OF COVERAGE.
_____ Policyholder Name _____ Employee Name _____ Social Security _____ Last First MI. I was given the opportunity to enroll in this plan of group health benefits offered by my employer and insured by Horizon Blue Cross Blue Shield of New Jersey Inc. I REFUSE the following.
Concerning that Group Health Plan on this Waiver of Coverage form. A health insurance waiver form will usually contain information regarding your request to waive access to a health insurance plan being offered to you. Any other inquiry related to your benefits or health plan Filing a Section 1557 Grievance by writing to the following address.
Employee Spouse and Children Coverage Spouse Coverage Children Coverage Reasons for Refusal Please indicate all that apply other group coverage sponsored by my employer. Box 29142 Hot Springs AR 71903 800-385-9088. SMALL EMPLOYER HEALTH BENEFITS WAIVER OF COVERAGE.
I was given the opportunity to enroll in this plan of group health benefits offered by my employer and insured by Aetna Inc. GROUP POLICY NO Signature of Employee EMPLOYEE NAME Last First MI. Department of Health and Human.
SMALL EMPLOYER HEALTH BENEFITS WAIVER OF COVERAGE CUSTOMER NAME I understand that if I later wish to enroll for any of the coverages refused I will be required to submit an Enrollment Form and coverage may be subject to a pre-existing conditions exclusions. The health insurance waiver form will include your declaration that you have been offered a plan however have chosen to refuse the health insurance coverage being offered to you. Department of Health and Human Services 200 Independence Avenue SW Room 509F HHH Building Washington DC.
That Group Health Plan on this Waiver of Coverage form.
 Free 9 Sample Employee Waiver Forms In Pdf Ms Word
Free 9 Sample Employee Waiver Forms In Pdf Ms Word
 Kaiser Group Health Insurance Waiver
Kaiser Group Health Insurance Waiver
 Can An Employee Decline Health Insurance Gusto
Can An Employee Decline Health Insurance Gusto
 Anthem Blue Cross Small Group Health Insurance Waiver Form
Anthem Blue Cross Small Group Health Insurance Waiver Form
 Http Thebenefitsourcellc Com Wp Content Uploads 2016 10 Oxfordsmgroupwaiver Pdf
Http Thebenefitsourcellc Com Wp Content Uploads 2016 10 Oxfordsmgroupwaiver Pdf
 Http Www Aetna Com Employer Plans Document Library Forms Nj Waiver Pdf
Http Www Aetna Com Employer Plans Document Library Forms Nj Waiver Pdf
 Employer Health Insurance Waiver Form Fill Online Printable Fillable Blank Pdffiller
Employer Health Insurance Waiver Form Fill Online Printable Fillable Blank Pdffiller
Fillable Online Visio Revised Benefits Waiver Ibc Form 6765 11 2013 Vsd Fax Email Print Pdffiller
 Fillable Online Small Employer Health Benefits Waiver Of Coverage Horizon Blue Fax Email Print Pdffiller
Fillable Online Small Employer Health Benefits Waiver Of Coverage Horizon Blue Fax Email Print Pdffiller
 Https Www Cigna Com Assets Docs Brokers And Consultants New Jersey Health Benefits Waiver5 Pdf
Https Www Cigna Com Assets Docs Brokers And Consultants New Jersey Health Benefits Waiver5 Pdf
 Fillable Online New Jersey Small Employer Health Benefits Waiver Of Coverage Fax Email Print Pdffiller
Fillable Online New Jersey Small Employer Health Benefits Waiver Of Coverage Fax Email Print Pdffiller
 Free 9 Sample Employee Waiver Forms In Pdf Ms Word
Free 9 Sample Employee Waiver Forms In Pdf Ms Word
 Free 9 Sample Employee Waiver Forms In Pdf Ms Word
Free 9 Sample Employee Waiver Forms In Pdf Ms Word
 Free 9 Sample Employee Waiver Forms In Pdf Ms Word
Free 9 Sample Employee Waiver Forms In Pdf Ms Word


Comments
Post a Comment