Silver 87 check out this plan for additional details. The SBC shows you how you and the plan would share the cost for covered health care services.
 Https Www Lacare Org Sites Default Files La1167 04 Lacc Eoc Silver 87 Hmo 2020 Pdf
Https Www Lacare Org Sites Default Files La1167 04 Lacc Eoc Silver 87 Hmo 2020 Pdf
Summary of Benefits and Coverage.

La care covered california silver 87 hmo. Silver 87 HMOCoverage for. 01012018 12312018 Summary of Benefits and Coverage. Silver 87 CommunityCare HMO.
Care Health Plan at 1- 855-270-2327. Silver 87 CommunityCare HMO. Information about the cost of this plan.
Beginning on or after 01012020Kaiser Permanente. This would be a good plan for a 40-year-old with an income between 150 18090 and 200 24120. The SBC shows you how you and the plan would share the cost for covered health care services.
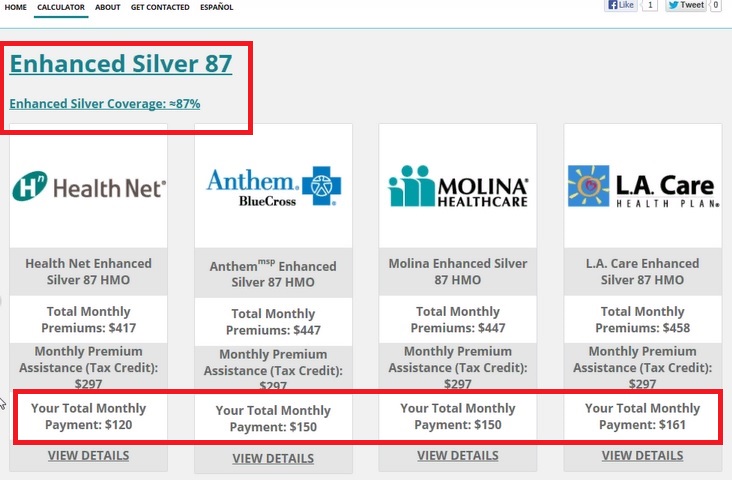
HMO Co-payments. Which one you qualify for depends on your household income. All Covered Members Plan Type.
70 73 87 and 94. Care Health Plan representatives are available 24 hours a day 7 days a week including holidays to help you. The SBC shows you how you and the plan would share the cost for covered health care services.
01012021 12312021. Silver 87 HMO Coverage Period. The SBC shows you how you and the.
01012017 12312017 Summary of Benefits and Coverage. Information about the cost of this. Health Net Silver 87 CommunityCare HMO Plan Overview Your Provider Network The Silver 87 CommunityCare HMO health plan utilizes the CommunityCare HMO provider network for covered benefits and services.
The Summary of Benefits and Coverage SBC document will help you choose a health plan. 1-888-4LA-CARE 1-888-452-2273 Provider Information. Since the service fees and deductible are low people with serious or chronic health conditions may wish to consider enrolling on a Silver 87 Plan if they are eligible.
One of the most popular Health Plans the Covered California Silver 87 plan includes a 50 individual Rx deductible 100 for families and minimal copays per script after the Rx deductible is met. The SBC shows you how you and the plan would share the cost for covered health care services. Or visit us at.
Silver 87 HMO Coverage Period. HMO 1 of 6 The Summary of Benefits and Coverage SBC document will help you choose a health plan. The SBC shows you how you.
The Summary of Benefits and Coverage SBC document will help you choose a health plan. 1-866-LACARE6 1-866-522-2736 Member Services. Summary of Benefits and Coverage.
Provider network for covered beneits and services. 1-888-839-9909 TTY 711 24 hours a day. Health Net of CA.
Silver 87 Rx Benefits. The Summary of Benefits and Coverage SBC document will help you choose a health plan. Department of Health and Human Services at 1-877-267-2323 x61565 or.
All Covered Members Plan Type. Covered CA_Silver 87 HMOCoverage for. The Silver 87 HMO health plan utilizes the.
Information about the cost of this plan. Individual Family Plan Type. Silver Coverage Silver Comes in Four Varieties.
Is available through Covered California in Los Angeles Orange and San Diego counties and. The Summary of Benefits and Coverage SBC document will help you choose a health plan. Silver 87 HMO.
Imaging CTPET scans MRIs 100 Not covered Prior Authorization is Required. LACC Silver 87 HMO LA. Silver 70 check out this plan for additional details.
Silver 87 CommunityCare HMO Coverage for. Health Care Coverage. Silver 73 check out this plan for additional details.
What this plan covers and What You Pay For Covered ServicesCoverage Period. Beginning on or after 01012019Kaiser Permanente. Health Net of CA.
30 for X-rays and diagnostic imaging. All Covered Members Plan Type. Beginning on or after 01012019.
1-855-270-2327 TTY 711 LA. Are fixed dollar amounts for example 15 you pay for covered health care usually when you receive the service. Preventive carescreeningimmunization No charge Not covered If you have a test Diagnostic test x-ray blood work 15 for laboratory.
What this plan covers and What You Pay For Covered ServicesCoverage Period. Health Net CALIFORNIA INDIVIDUAL FAMILY PLANS. What this Plan Covers What it Costs.
Care Health Plan Silver 87 HMO This health insurance plan is for individuals and families with an annual gross income between 151 to 200 of the federal poverty level FPL who also meet other applicable guidelines. Health Net of CA. Use the Shop and Compare Tool to see if you can get extra savings with Silver 73 87 and 94.
Generally adults with an income of just above 138 to 250 of the Federal Poverty Level may qualify for enhanced benefits. Health Net of California Inc. Other coverage options may be.
You can view the Glossary at. Plan Overview Silver 87 CommunityCare HMO. Care CoveredDirect Member Services.
Information about the cost of this plan called the premium will be. CommunityCare HMO is available through Covered CA in Los Angeles Orange and San Diego counties and parts of. Beginning on or after 01012021.
Care at 1 888 HMO-2219 1-888-466-2219 or. Individual Family Plan Type. What this Plan Covers What it Costs Coverage for.
Health Net of California Inc. To qualify for an Enhanced Silver 87 Plan the application must be submitted through Covered California and the individual must meet Covered California income limits.
 Http Www Lacare Org Sites Default Files La0924b 2019 Lacc Sbc Silver 87 1018 Pdf
Http Www Lacare Org Sites Default Files La0924b 2019 Lacc Sbc Silver 87 1018 Pdf
 Https Www Lacare Org Sites Default Files La0921d 2021 Lacc Silver 87 Hmo Sbc Pdf
Https Www Lacare Org Sites Default Files La0921d 2021 Lacc Silver 87 Hmo Sbc Pdf
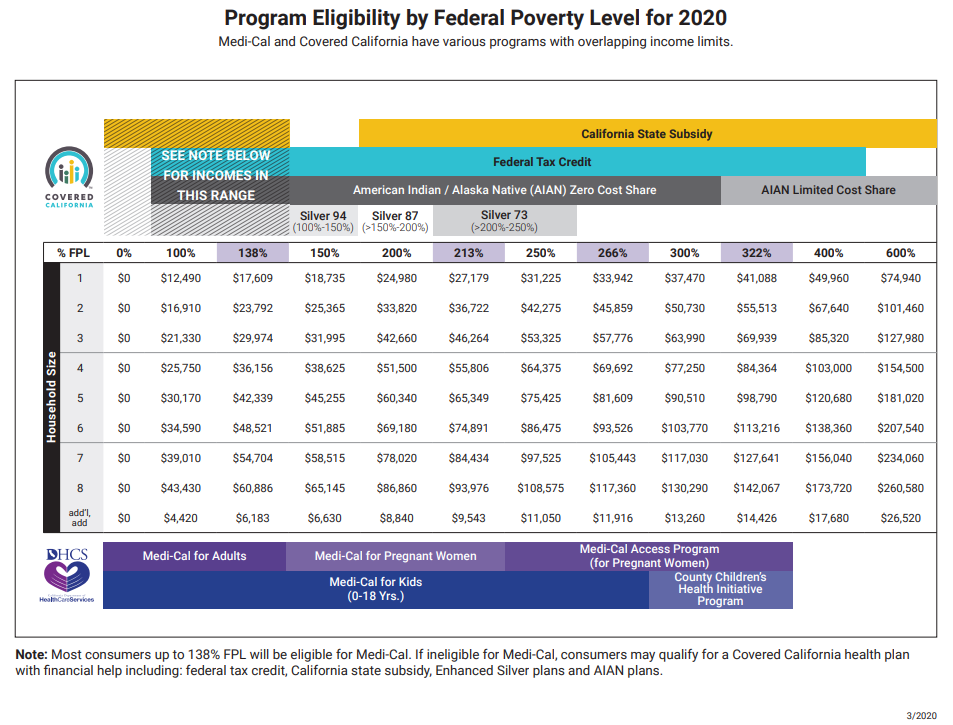 Fpl Federal Poverty Income Chart Covered Ca Subsidies Tax Credits
Fpl Federal Poverty Income Chart Covered Ca Subsidies Tax Credits
 2
2
 Health Insurance Companies In California Covered California
Health Insurance Companies In California Covered California
 Lacc Silver 87 Hmo L A Care Health Plan
Lacc Silver 87 Hmo L A Care Health Plan
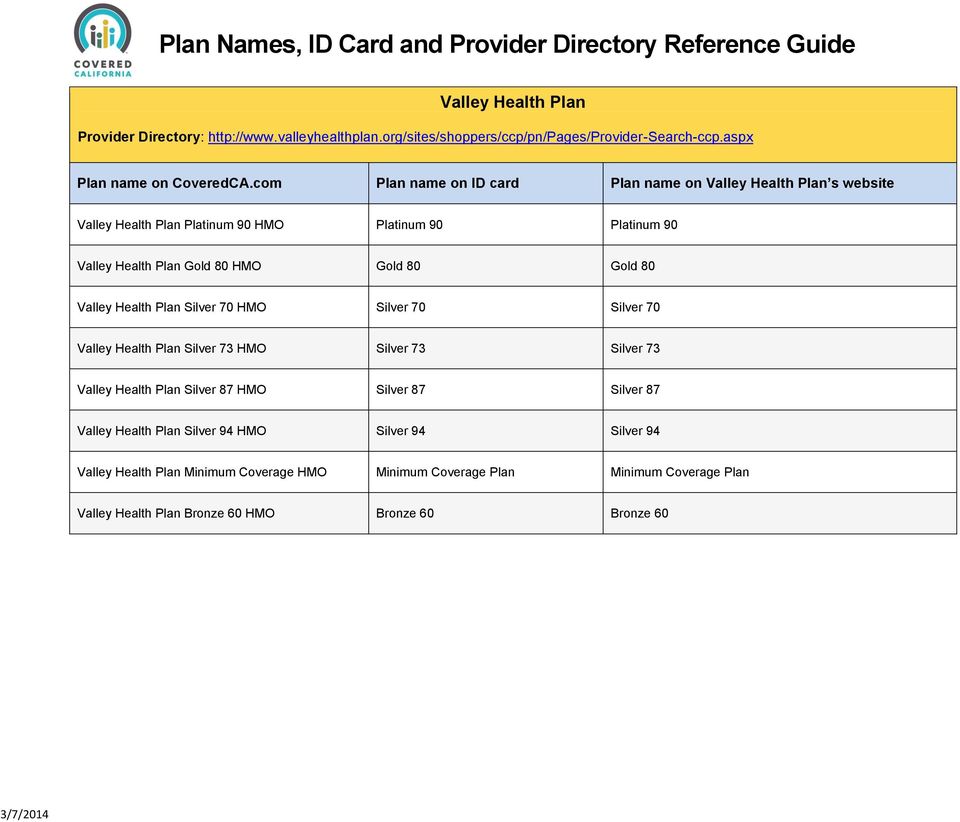 Plan Names Id Card And Provider Directory Reference Guide Pdf Free Download
Plan Names Id Card And Provider Directory Reference Guide Pdf Free Download
 Plan Names Id Card And Provider Directory Reference Guide Pdf Free Download
Plan Names Id Card And Provider Directory Reference Guide Pdf Free Download
 Health Agents To Get Mobile App From Covered California
Health Agents To Get Mobile App From Covered California
 Covered California Silver 87 Plans Health For California
Covered California Silver 87 Plans Health For California
 Https Www Lacare Org Sites Default Files L A Care Covered Silver 87 Hmo Evidence Of Coverage 0 Pdf
Https Www Lacare Org Sites Default Files L A Care Covered Silver 87 Hmo Evidence Of Coverage 0 Pdf
 Http Lacare Org Sites Default Files Universal La0967 2019 Plans At A Glance 0818 Pdf
Http Lacare Org Sites Default Files Universal La0967 2019 Plans At A Glance 0818 Pdf
Https Www Lacare Org Sites Default Files La0924b 2018 Lacc Sbc Silver 87 Hmo 508c 0917 Pdf
 Health Net Of California Imk
Health Net Of California Imk


Comments
Post a Comment